A startup used Enter to create certified-mail appeals with real medical guidelines
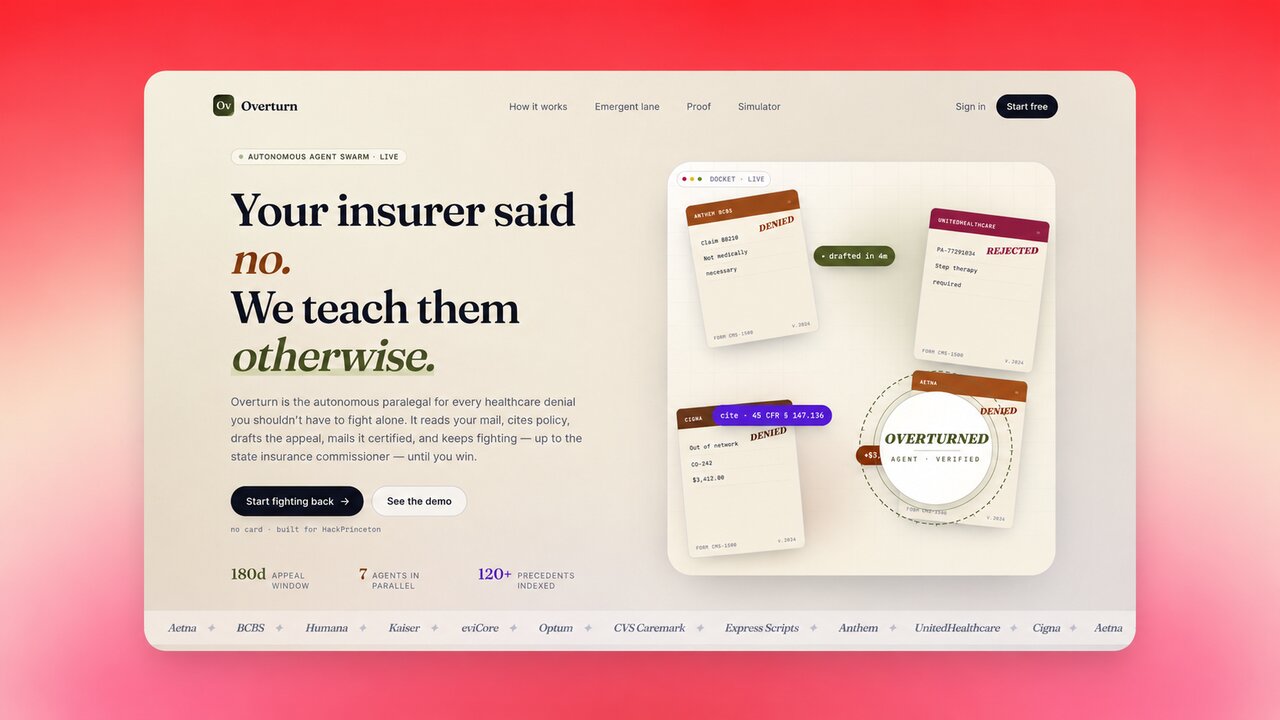
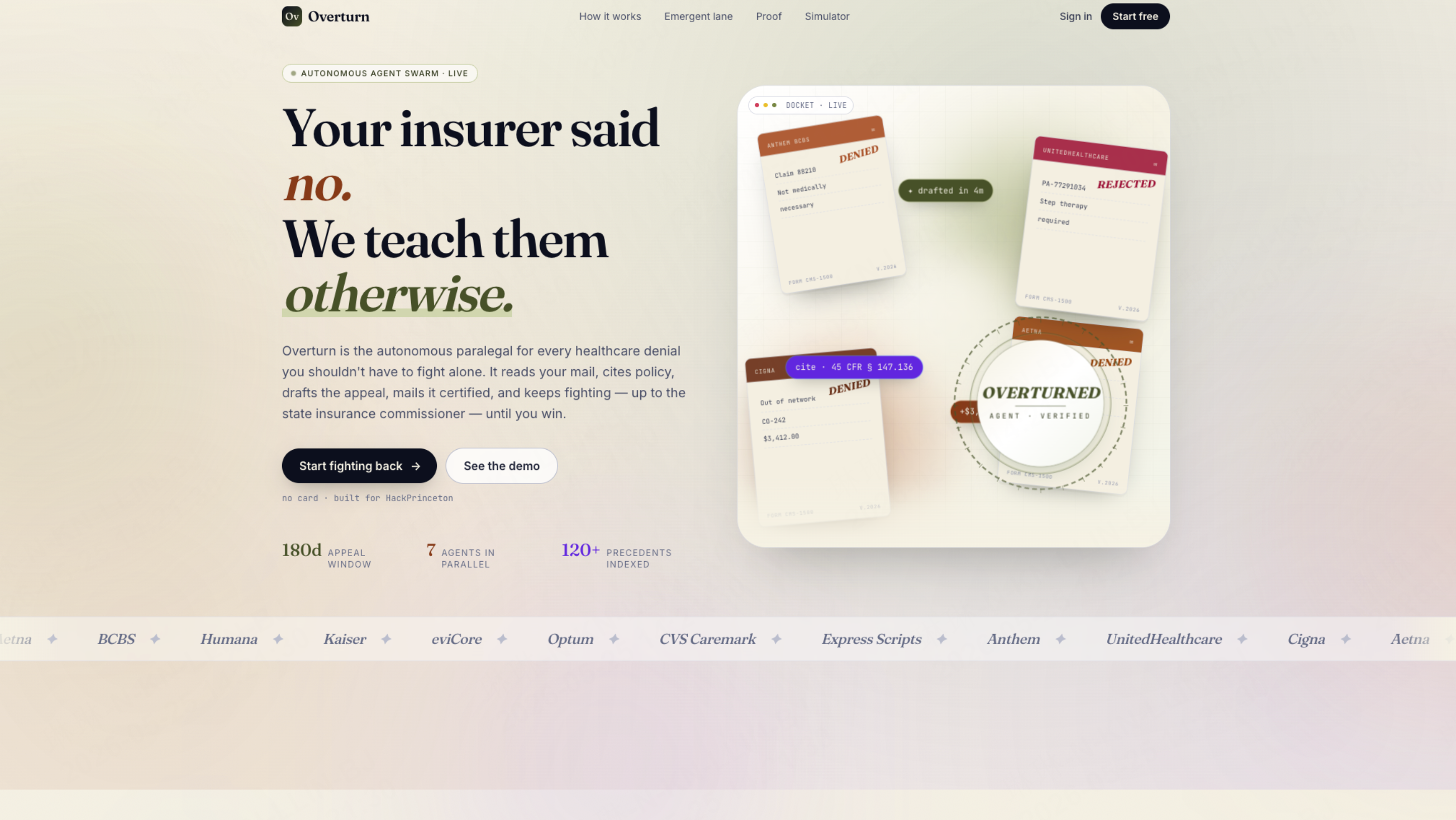
81.7% of insurance denial appeals succeed—but fewer than 1% ever fight back. Overturn files certified-mail appeals with real medical guidelines in 60 seconds.
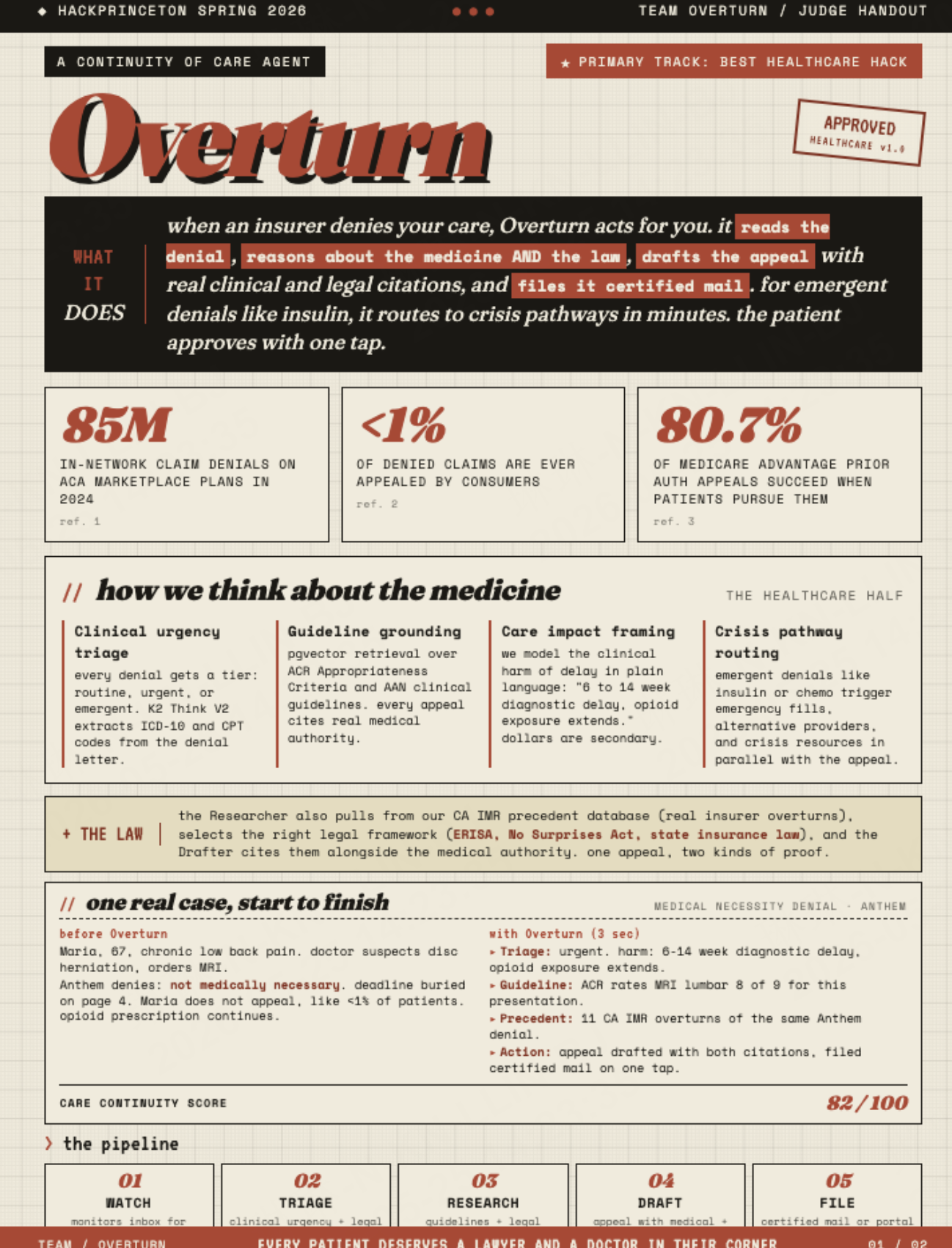
In 2024, insurers denied 85 million in-network claims on the ACA marketplace. Fewer than 1% were ever appealed. And when patients actually fight back? 81.7% of prior authorization denials get overturned.
The math is worth sitting with. The fight works. Most people just never fight.
Not because they do not care. Because the asymmetry is by design. Insurers have entire teams of lawyers, AI models, and clinical reviewers who designed the denial. Patients have a letter, a deadline, and hold music. By the time most people figure out that an appeal is even possible — that the denial is not the final word legally — the window has usually passed.
We were at the Princeton Hackathon 2026 to support teams to ship a real product in 36h, and the team behind Overturn decided to change the math.
What Overturn Does
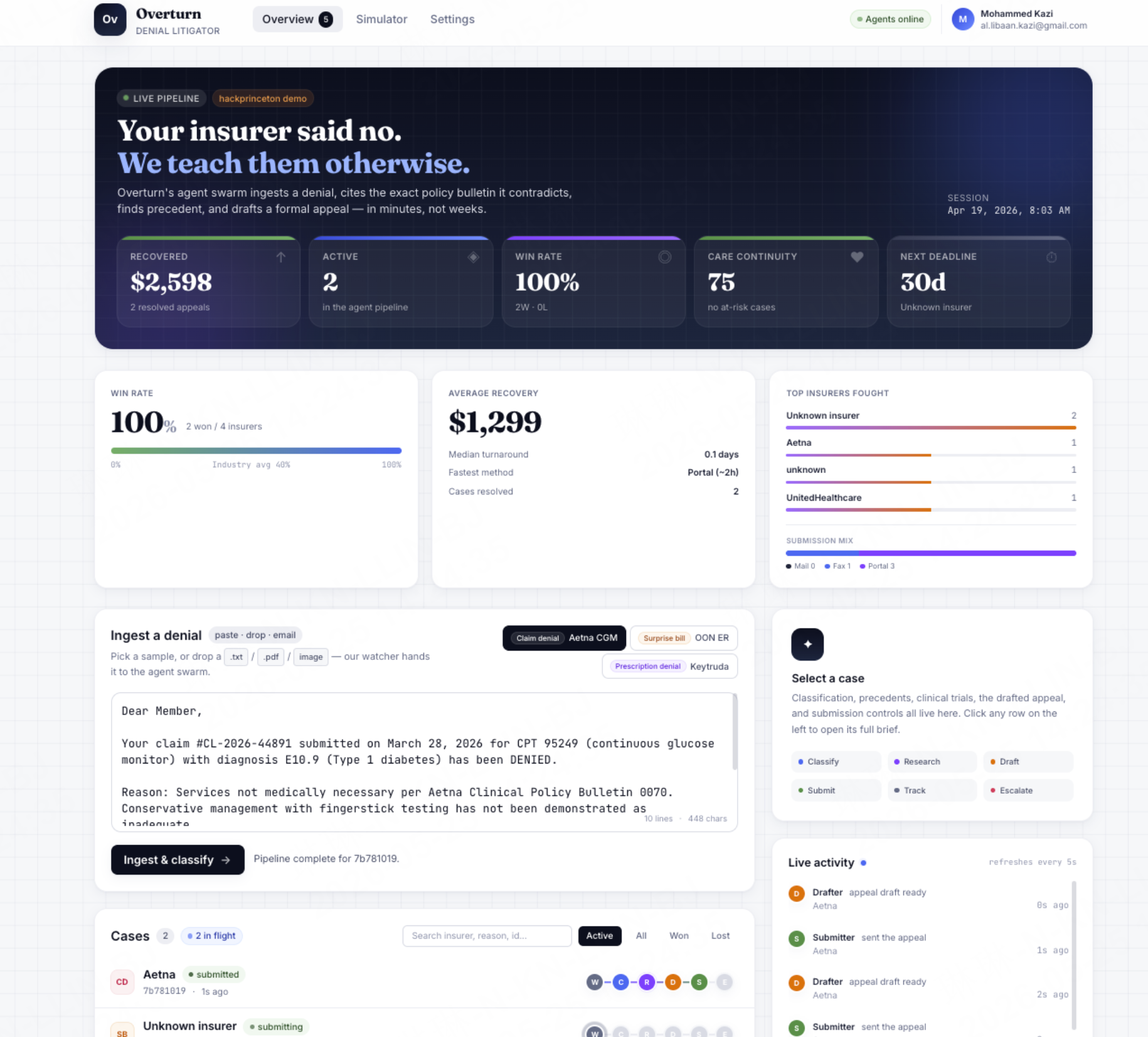
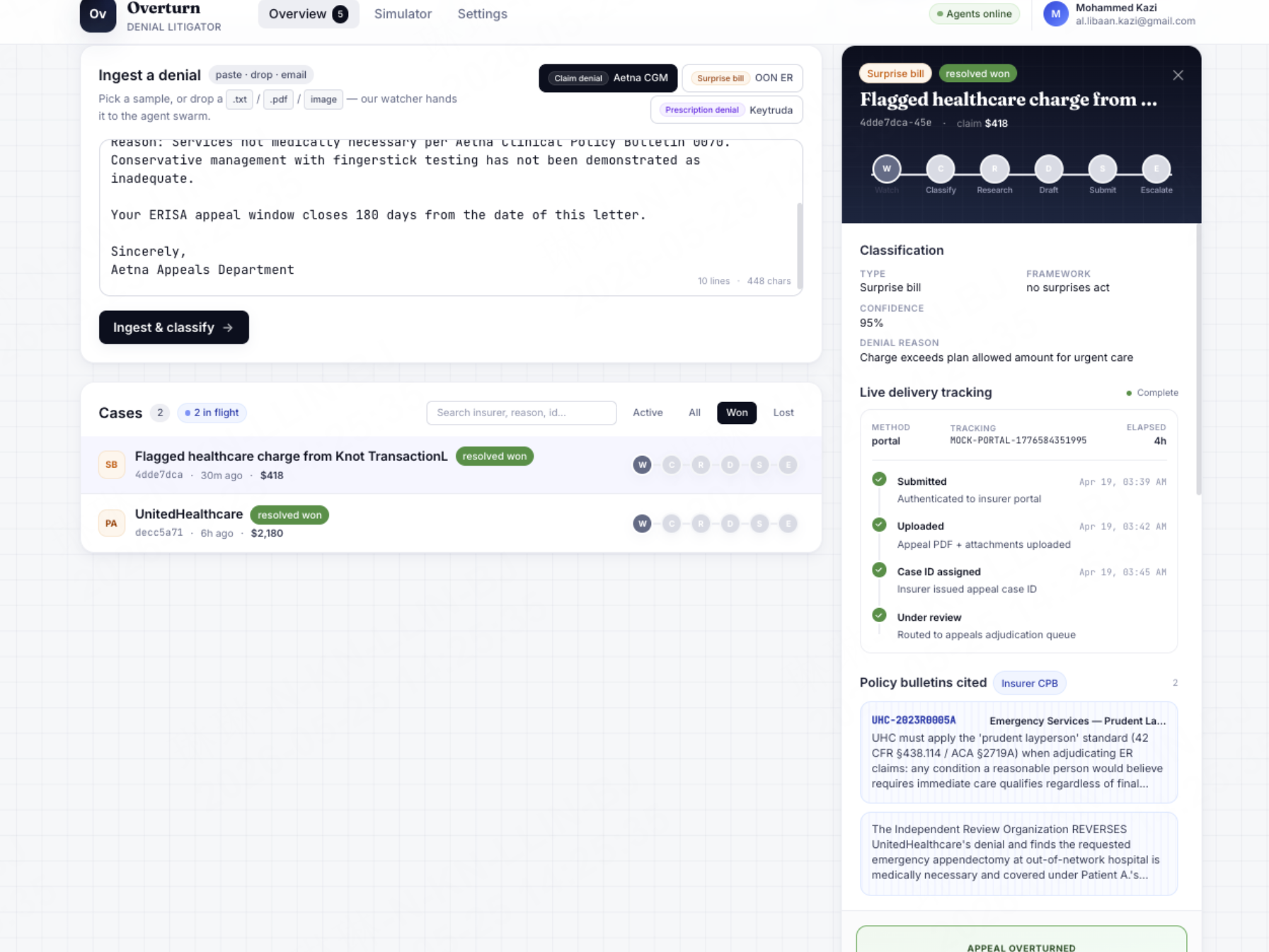
Drop in a denial letter. Sixty seconds later, a certified-mail appeal is in the postal pipeline — with a real tracking number, a real medical guideline cited, a real legal precedent cited, and the specific clinical harm of the denial spelled out in plain language.
Not a draft. Not a template. A filed appeal.
The sequence:
| Step | What happens |
| Read | Diagnostic codes, procedure codes, denial reason extracted from the letter |
| Triage | Clinical urgency scored. Legal framework selected. |
| Research | Medical guidelines and legal precedents pulled in parallel |
| Harm model | Denial translated into clinical consequences — not dollar amounts |
| Draft | Formal appeal generated with both authority types cited |
| File | Certified mail submitted. Tracking number returned. |
Patient approves. Overturn handles everything else.
Why This Is Healthcare, Not Paperwork
Every other appeal tool stops at "here is a draft letter, good luck." They treat denials like paperwork problems. Denials are medical problems. Medical arguments are the ones that win.
Three things make the distinction real.
Clinical guideline grounding. Every appeal cites real medical authority — not summaries, not paraphrases. The actual guidelines from the bodies that govern medical necessity decisions. When a radiologist's order is denied, the appeal does not argue general reasonableness. It cites the specific appropriateness rating for the exact clinical presentation.
Care impact framing. The agent argues patient harm, not patient costs.
| ❌ Financial argument | ✅ Clinical argument |
| "$4,237 in out-of-pocket expenses" | "Estimated 6–14 week diagnostic delay. Opioid exposure extends with each week. Conservative management already failed at 12 weeks per PT records." |
That is the argument that wins.
Urgency triage. Not every denial is equal. Overturn does not treat them equally.
| Tier | Example | What the agent does |
| 🟢 Routine | Elective imaging, PT sessions | Standard appeal flow |
| 🟡 Urgent | Suspected disc herniation, chronic pain | Appeal + surface alternative providers |
| 🔴 Emergent | Insulin, chemotherapy, oxygen | Crisis pathway — emergency fill laws, parallel filing, acts in minutes |
An insulin denial is not a routine denial with a faster timer. It is a medical emergency. The agent knows the difference.
One Real Case
Meet Maria. 67 years old. Chronic low back pain for two years. Her doctor suspects a disc herniation and orders an MRI. The insurer denies: not medically necessary.
Maria, like 99% of patients, does not appeal. The opioid prescription continues. The disc gets worse.
With Overturn, here is what happens in under three seconds:
- Triage: urgent. Estimated 6–14 week diagnostic delay. Opioid exposure extends with each week.
- Guideline: clinical appropriateness rating for MRI in this exact presentation is 8 out of 9 — one of the highest ratings the relevant medical body assigns.
- Precedent: eleven documented overturns of the identical denial from the same insurer, all publicly reported.
- Draft: formal appeal generated, both citations inline, clinical harm framed in medical language.
- Filed. Certified mail. Tracking number returned.
The team does not optimize for appeal wins. They optimize for continuity of care.
How They Built It
The architecture reflects the premise: not one system wearing multiple hats, but a genuine swarm — six specialized agents, each with a defined role, coordinating through shared state and a clean event system.
The decision to separate concerns from the start paid back across the full 36-hour build. The first agent took eight hours to get right. Adding the sixth took two. Infrastructure discipline at the beginning made every subsequent hour faster.
Two problems shaped the project more than any other.
Retrieval quality. Four major medical bodies publish guidelines in formats that do not speak to each other — appropriateness ratings, narrative evidence summaries, decision trees, letter grades. Building a normalization layer that made all four query-compatible while preserving their original format was one of the harder problems the team solved. It is also the product. The appeal is only as strong as the evidence it cites — and that evidence only surfaces if the retrieval actually works.
Dual-source drafting. Early appeal drafts leaned toward whichever source came back strongest. If legal precedent dominated, the appeal read like a legal brief. If clinical evidence dominated, it read like a physician's note. Neither was right. The fix: a structured output that required both authority types to be explicitly filled before any draft could generate. The appeal cannot be written unless the clinical argument and the legal argument are both present.
Enter.pro credits gave the team the velocity to stay focused on the hard problems during the build — keeping infrastructure friction low across a 36-hour sprint where every hour counted.
What They Are Proudest Of
The live demo moment: a real certified-mail tracking number returned on stage, in under two seconds. Not a simulated output. Not a prototype response. A filed appeal, with a postal tracking number, generated in real time.
That is not a demo feature. That is the product working as designed.
This Is the Tenth Project We Have Written About From HackPrinceton
405 participants. 36 hours. We have kept following what came out of that weekend because the quality of thinking has kept earning the attention.
Overturn earns its place in this series because the problem it is addressing is both technically difficult and genuinely consequential. 85 million denied claims. Fewer than 1% appealed. 81.7% of those overturned. The gap is not ignorance — most people know they could fight. The gap is the asymmetry. Overturn closes it.
What Comes Next
The immediate roadmap focuses on the highest-volume denial categories: Medicare Advantage and Medicaid, where prior authorization denial rates are highest. A provider-side version is planned — physicians spend 13 hours per week on prior authorization paperwork; the same system that helps patients can give that time back to the doctors who treat them.
An expanded precedent database will cover more states and more specialty guidelines. A caregiver permissions model is next for the adult children who are often the ones managing these appeals on behalf of aging parents.
The goal is the same at any scale.
Every patient deserves both a doctor and a lawyer in their corner when the insurer sends the letter. Overturn puts both there.
The team behind this built : Khushi Motwani | Al-Libaan Kazi
Missed the earlier volumes? → Vol. 1 — Heritage in Pixels → Vol. 2 — Terra Zone AI → Vol. 3 — reAgent → Vol. 4 — TaleTailor → Vol. 5 — LEGR → Vol. 6 — PolyPath → Vol. 7 — EcoThread→ Vol. 8 — Aletheia → Vol. 9 — Synova